Classifications
I) clinical cure:
drugs used to treat the acute attack of malaria by acting on the erythrocyte stage of the parasite
- chloroquine-sensitive malaria: Chloroquine
- chloroquine-resistance malaria:
- -Quinine - ***acute ; Cinnchonism | Black water fever
- -Mefloquine; least side effects among the group mild & moderate cases & chemoprophylaxis
- Y Folate AntagonistsAntifolate;(pyremethamine; acts on liver stage ,progunail,Sulphonamides):
- -sulphadoxine
- -combination: Fansidar = sulphadoxine + pyremethamine Fansimaf = sulphadoxine + pyremethamine + mefloquine
II) chemoprophylaxis:
-
clinical prophylaxis: Chloroquine, proguanil, & fansidar = sulphadoxine + pyremethamine suppress the clinical manifestation of malaria by killing parasite as soon as they reach the RBCs .
-
antirelapse therapy: Primaquine in P.vivax and ovale only by killing the dormant stage in liver;
-
prevent transmission: Primaquine + folate antagonists; progunail ,pyremethamine by killing the gametocytes:
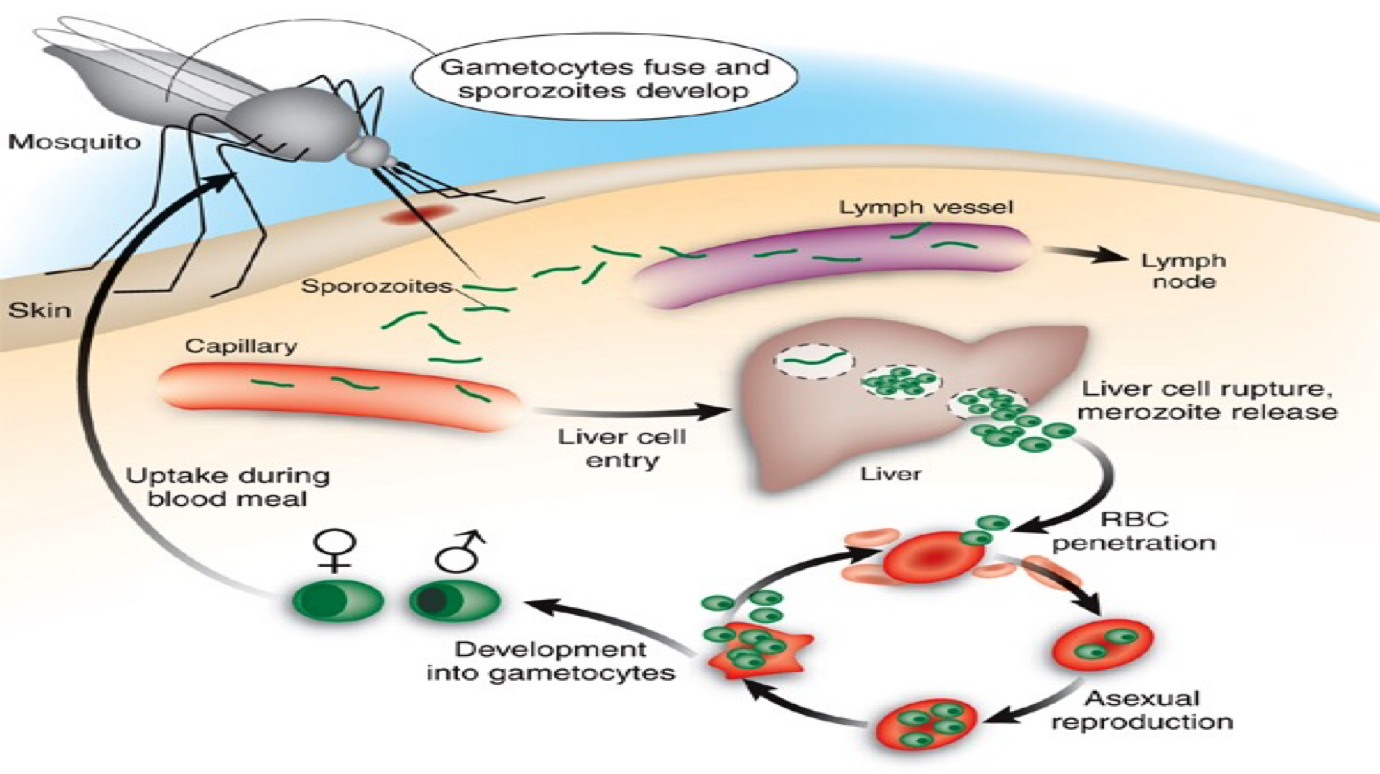
PATHOPHYSIOLOGY and life cycle:
- Anopheles mosquito inoculates sporozoites to human .
- Sporozoites invade liver cells ( primary tissue phase).
- Merozoites released from liver & invade erythrocytes .
- Merozoites multiply, red cell enlarges ( blood schizont).
- blood schizont ruptures, merozoites invade more RBCs.
- Repeated cycles cause clinical illness, fever, etc.
- In P. vivax & P. ovale some merozoite invade liver cells Z ( secondary tissue phase) & become dormant ( hypnozoites ) hypnozoites may develop again and cause relapse.
- In P. falciparum & P. malariae no second liver phase.
- Some merozoite — gametocytes— mosquito — sporozoites
Common symptoms
Recurrent fever and chills, splenomegaly
Life cycle of malaria