Pyogenic liver abscess
Routes of infection
- Biliary system (the commonest)
- Portal system (e.g. acute appendicitis)
- Hepatic artery from any septic focus in the body (infective endocarditis)
- Contagious organ (e.g. empyema gallbladder)
- Trauma (penetrating or blunt)
- Idiopathic (unknown source)
Clinical features
Possible sign and symptoms:
- Pyrexia of unknown origin
- There is some times a history of sepsis elsewhere, particularly within the abdomen
- Pain in the right upper quadrant
- Swinging pyrexia, rigors, marked toxicity
- Jaundice
- The liver is often enlarged and tender
Investigations
-
blood tests: complete blood count will show leukocytosis and liver function tests are deranged
-
imaging: chest x-ray will show elevation of diaphragm and basal lung lobe collapse. ultrasound and CT scan is used to define the abscess.
-
ERCP: may be useful if biliary obstruction is thought to be responsible.
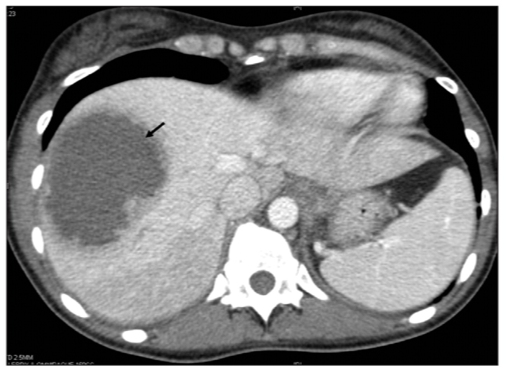
CT scan abdomen showing pyogenic abscess in the right lobe of the liver
Management
Untreated abscess often prove fatal because of spread within the liver to multiple sites, and because of septicemia.
- Intravenous antibiotics should be given to all patients
- Percutaneous Drainage U/S GUIDED of the abscess: percutaneous drainage under ultrasound or CT scan guidance or surgical drainage if percutaneous drainage failed
- Multiple small abscess may require prolonged treatment with antibiotics for up to 8 weeks.
- Investigation is required to detect the source (e.g. colonoscopy, ERCP, CT scan abdomen)