Antidepressants
Antidepressants Indications: Unipolar and bipolar depression, organic mood disorders, schizoaffective disorder, anxiety disorders including OCD, panic, social phobia, PTSD, premenstrual dysphoric disorder and impulsivity associated with personality disorders.
General guidelines for antidepressant use
- Antidepressant efficacy is similar so selection is based on past history of a response, side effect profile and coexisting medical conditions.
- There is a delay typically of 2-4 weeks after a therapeutic dose is achieved before symptoms improve.
- If no improvement is seen after a trial of adequate length (at least 2 months) and adequate dose, either switch to another antidepressant or augment with another agent.
Antidepressant Classifications
- Tricyclics (TCAs)
- Monoamine Oxidase Inhibitors (MAOIs)
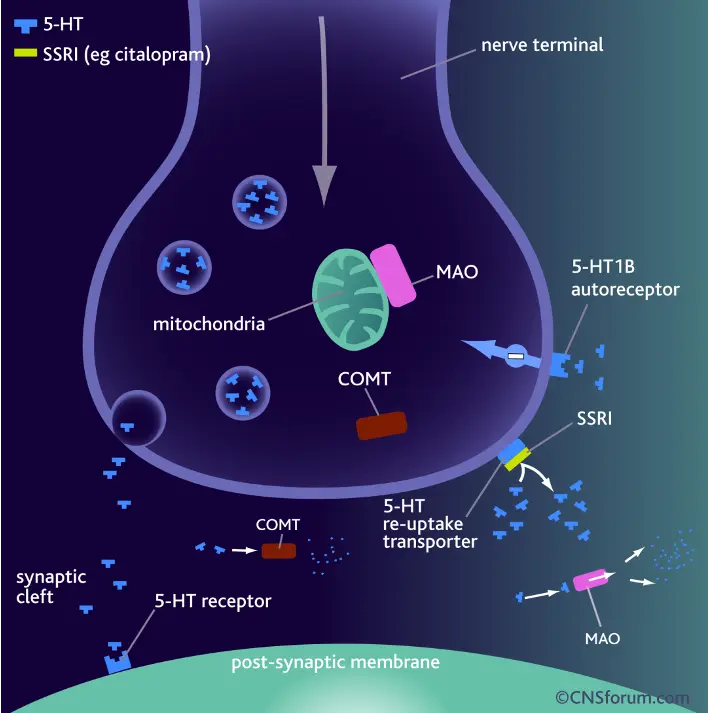
- Selective Serotonin Reuptake Inhibitors (SSRIs)
- Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
- Novel antidepressants

Case 1
Case 1
- Susie Q has a nonpsychotic unipolar depression with no history of hypomania or mania. She has depressed mood, hyperphagia, psychomotor retardation and hypersomnolence. What agent would you like to use for her?
- Establish dx: Major depressive disorder
- Target symptoms: depression, hyperphagia, psychomotor retardation and hypersomnolence
- For a treatment naive patient start with an SSRI.
- Using the side effect profile as a guide select an SSRI that is less sedating. Good choices would be Citalopram, Fluoxetine or Sertraline. Buproprion would also have been a reasonable choice given her hypersomnolence, psychomotor retardation and hyperphagia.
- Less desirable choices include Paxil and Mirtazapine because of sedation and wt gain.
- Not a duel reuptake inhibitors because she is treatment naïve and may not need a “big gun”.
- Not a TCA because of side effects
Case 2
Case 2
- Billy bob is a 55 year old diabetic man with mild HTN and painful diabetic neuropathy who has had previous depressive episodes and one suicide attempt. He meets criteria currently for a major depressive episode with some anxiety. He has been treated with paroxetine, setraline and buproprion. His depression was improved slightly with each of these meds but never remitted. What would you like to treat him with?
- Establish dx: Major depressive disorder with anxious features
- Target symptoms: depressive sx, anxiety and possibly his neuropathic pain
- Assuming he received adequate trials previously would move on to a duel reuptake inhibitor as he had not achieved remission with two SSRIS or a novel agent.
- Given his mild HTN would not choose Venlafaxine. TCA’s can help with neuropathic pain and depression however not a good choice given the SE profile and lethality in overdose. Duloxetine is a good choice since it has an indication for neuropathic pain, depression and anxiety. Three birds with one stone!!
- Keep in mind Duloxetine is a CYP2D6 and CPY1A2 inhibitor and has potential drug-drug interactions.