Ulnar Nerve Injury

Claw-hand deformity
in ulnar lesions
Interosseous
atrophy
Sensory distribution

KEY
| Red | Posterior (dorsal) interossei (4) |
|---|---|
| Blue | Posterior interossei (3) |
| Green | Ulnar lumbricales (2) |
Ulnar Nerve Injury
- Common sites for injury
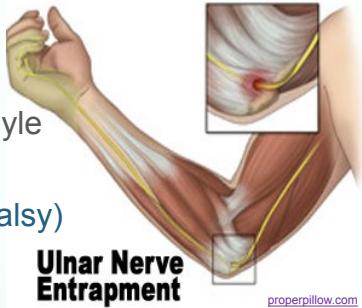
- At the elbow
- Fracture of the medial epicondyle
- Cubitus valgus
- (causing tardy ulnar nerve palsy)
- Ulnar nerve entrapment
- At the wrist
- Cut wound

Ulnar Nerve Injury
Common Sites of Injury
Elbow Region:
- Medial epicondyle fractures: Direct trauma or valgus stress
- Cubitus valgus deformity: Chronic stretching leading to tardy ulnar nerve palsy
- Cubital tunnel syndrome: Compression at the elbow
Wrist Region:
- Guyon’s canal compression: Compression at the wrist
- Lacerations: Direct penetrating injuries
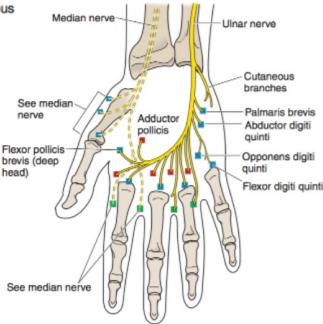
Motor Deficits
Muscles Affected:
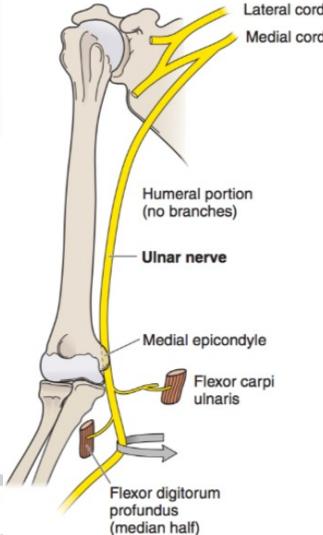
- Flexor carpi ulnaris: Wrist flexion and ulnar deviation
- Medial half of flexor digitorum profundus: Distal interphalangeal joint flexion of ring and little fingers
- All interossei muscles: Finger abduction and adduction
- Third and fourth lumbricals: Metacarpophalangeal joint flexion with IP extension
Clinical Manifestations:
- Loss of finger abduction and adduction: Cannot spread or close fingers properly
- Intrinsic muscle wasting: Visible atrophy of interossei and hypothenar muscles
- Weakness of grip: Due to loss of intrinsic stabilization

Sensory Deficits
Distribution:
- Sensory loss: Medial 1½ fingers (little and half of ring finger)
- Both palmar and dorsal surfaces: Complete sensory involvement
- Medial forearm: Variable sensory loss in proximal lesions
Characteristic Deformities
Claw Hand Deformity:
- Extended metacarpophalangeal joints: Due to unopposed extensor action
- Flexed interphalangeal joints: Due to unopposed flexor action
- Most prominent in ring and little fingers: Ulnar distribution


Ulnar Paradox
Pathophysiology:
-
Low ulnar nerve lesions (at wrist):
- More pronounced clawing of ring and little fingers
- All flexors remain functional, pulling fingers into claw position
-
High ulnar nerve lesions (at elbow):
- Less obvious clawing deformity
- Paralysis of ulnar half of FDP reduces finger flexion, partially preventing claw hand
Clinical Significance:
- Helps localize level of nerve injury
- Important for prognosis and surgical planning