Practice Cases
- Now you have the terms you need
- Let’s practice your descriptions with cases
- Do the best you can – like learning any new language it takes practice!
Case One: Mr. F
Case One: History
- HPI: Mr. F is a 32-year-old man who presents to his primary care provider with “blotches” on his upper back, chest, and arms for several years.
- They are more noticeable in the summertime.
- PMH: shoulder pain from an old sports injury
- Allergies: none
- Medications: NSAID as needed
- Family history: not contributory
- Social history: auto mechanic
- ROS: negative


-
Are these lesions elevated, flat, or depressed?
-
If you don’t feel an elevation or depression as your finger runs across the skin, they are flat
- Small, flat lesions are called macules
-
How else can you describe them?
- What size are they? 3 to 10 mm
- What shape are they? Round to oval
- What color are they? Pink to tan
- How regular and distinct is the border? Sharp, irregular borders
- How are they configured? Separate, in no particular pattern
- How are they distributed? On the upper chest, back, and flexures of arms
Skin Exam Summary and Diagnosis
- Mr. F’s skin exam shows:
- Multiple 3 to 10 mm pink to tan-colored, round, flat lesions with sharp, irregular borders and varying sizes on his upper chest, back and flexures of the arms.
- Small (< 1cm) flat lesions are called macules
- In this case, the primary lesion is a macule
Diagnosis Details
- Dr. D performs a potassium hydroxide exam and based on the findings, diagnoses Mr. F with tinea versicolor. The primary lesion in tinea versicolor is a macule
Which of the following answers are correct? (More than one may be correct.) Answer: b & d
- Macules can: a. Feel raised (these are papules or plaques) b. Feel flat c. Contain fluid (these are vesicles or bullae) d. Be any shape
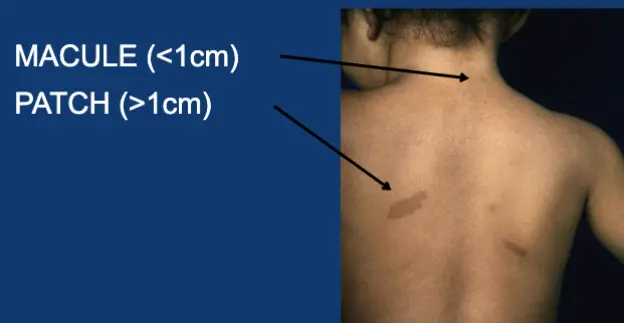
Review: Macule vs Patch
MACULE (<1cm)
PATCH (>1cm)
Case Two: Mr. K
Case Two: History
- HPI: Mr. K is a 36-year-old man who presents with four years of itchy, flaky spots on his elbows, knees, and lower back. They have not improved with moisturizers.
- PMH: none
- Allergies: none
- Medications: none
- Family history: father died from heart attack at age 68
- Social history: delivery truck driver
- Health-related behaviors: drinks 2-3 beers a week
- ROS: negative


- How would you describe these skin findings?
- Be as detailed as you can be!
- Imagine running your finger over them.
- These are raised
- Large (>1cm), plateau- like, raised lesions are called plaques
- How else can you describe them?
- Size? 3 to 10 cm
- Shape? Round to geographic (like outlines on a map)
- Color? Pink
- Sharp borders? Sharply circumscribed
- Texture? Scaly
- Configuration? Symmetrical
- Distribution? Extensor surfaces (knees, elbows), back, gluteal cleft
Case Two: Diagnosis
- Mr. K’s skin exam shows:
- Several 3-10 cm pink round sharply circumscribed scaly plaques on his extensor elbows, knees, lower back, and gluteal cleft
- Mr. K has psoriasis.
- The primary lesion in this case of psoriasis is a plaque because it is elevated and over 1 cm in diameter.
Review: Papule vs Plaque
PAPULE (<1cm)
PLAQUE (>1cm)

Case Three: Mr. B
Case Three: History
- HPI: Mr. B is a 28-year-old man who presents with four days of pain and blisters on his left chest.
- PMH: none
- Allergies: none
- Medications: none
- Family history: noncontributory
- Social history: single; works as a personal trainer
- ROS: negative


Case Three, Questions
- How would you describe these skin findings?
- Are these lesions raised, flat, or depressed? These are raised
- Do they have fluid in them? They also have fluid in them
- Remember - small, raised, fluid-filled lesions are called vesicles
Case Three: Descriptive Questions
- How else can you describe them?
- Size?2 – 5 mm
- Shape? Round to oval
- Color? Clear, with a background erythematous patch
- Texture? Fluid-filled
- Configuration? Grouped vesicles
- Distribution? Unilateral dermatomal distribution on the left chest
Distribution / Configuration Explanation
- Part of describing lesions is noting distribution and configuration
- Distribution means location(s) on the body
- Configuration means how the lesions are arranged or relate to each other
- Lesions are grouped but also follow a linear pattern around the trunk
- This is an example of a segmental or dermatomal distribution
Diagnosis
- Mr. B’s skin exam shows:
- Grouped 2-5 mm vesicles on an erythematous base in a unilateral, dermatomal configuration on the left chest
- Small, fluid-filled lesions are called vesicles
- Mr. K has shingles. The primary lesion in shingles is a vesicle.