Hodgkin’s Lymphoma
Overview
Hodgkin’s lymphoma is a malignancy arising in the lymphoid tissues (mainly lymph nodes). The cell of origin is the “B” lymphocyte.
Etiology: Epstein-Barr virus is thought to play a major role in most cases.
Epidemiology
Hodgkin’s lymphoma has a peak incidence in two age groups (bimodal):
- Young adulthood (in the 20s)
- Above 50
Signs and Symptoms
-
Lymph Node Enlargement:
- Commonest Feature
- Most common is enlargement of axillary, cervical, supraclavicular & inguinal nodes
- Nodes are painless and rubbery
- Nodes become acutely painful after alcohol intake (2-3% of patients)
-
Systemic Features (B Symptoms):
- Low-grade fever
- Night sweats
- Weight loss (at least 10% of body weight in less than 6 months)
- Note: B Symptoms may or may not be present.
- Pruritus
-
Other Findings:
- Splenomegaly (often seen)
- Hepatomegaly (possible but not very common)
- Features of nephrotic syndrome (pathology in the glomerulus is minimal change disease) Z
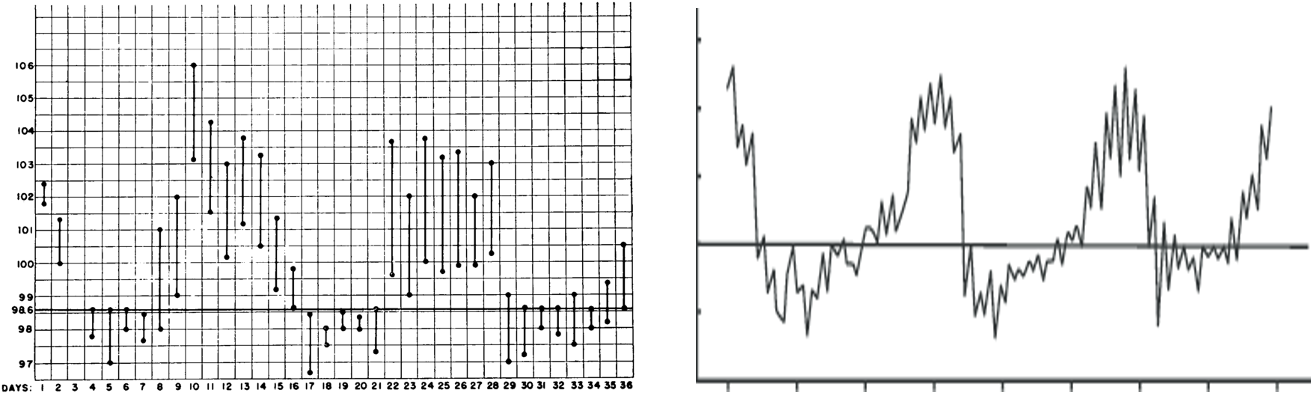
Pel-Ebstein Fever
- A cyclic pattern of fever, rarely seen in Hodgkin’s patients
- Fever present for a few days, then absent for a few days (cycle continues)
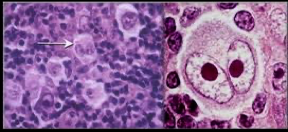
Diagnostic Feature
The diagnostic feature is the presence of malignant Reed-Sternberg cells (R-S cells), seen on lymph node biopsy.
- Large cell with two nuclei, looking like “owl eyes”
Classification of Hodgkin’s Lymphoma
-
Classic Hodgkin’s Lymphoma (Most Cases):
- Lymphocyte-rich: RS cells + excess lymphos.
- Lymphocyte-depleted: RS cells plus very few lymphos
- Mixed cellularity: Almost equal number of RS cells and lymphos
- Nodular sclerosis: RS cells plus lymphos plus fibrous tissue
-
Nodular Lymphocyte Predominant Hodgkin’s Lymphoma (Only 10% of Cases)
Diagnosis & Workup
- Diagnosis: Confirmed by lymph node biopsy showing R-S cells. - After diagnosis, workup is done for staging the lymphoma, so that treatment options can be decided
- Workup:
- Routine blood tests (CBC, electrolytes, etc.)
- Imaging:
- Whole body imaging (CT, MRI, or PET scan) to determine affected lymph nodes.

- Whole body imaging (CT, MRI, or PET scan) to determine affected lymph nodes.
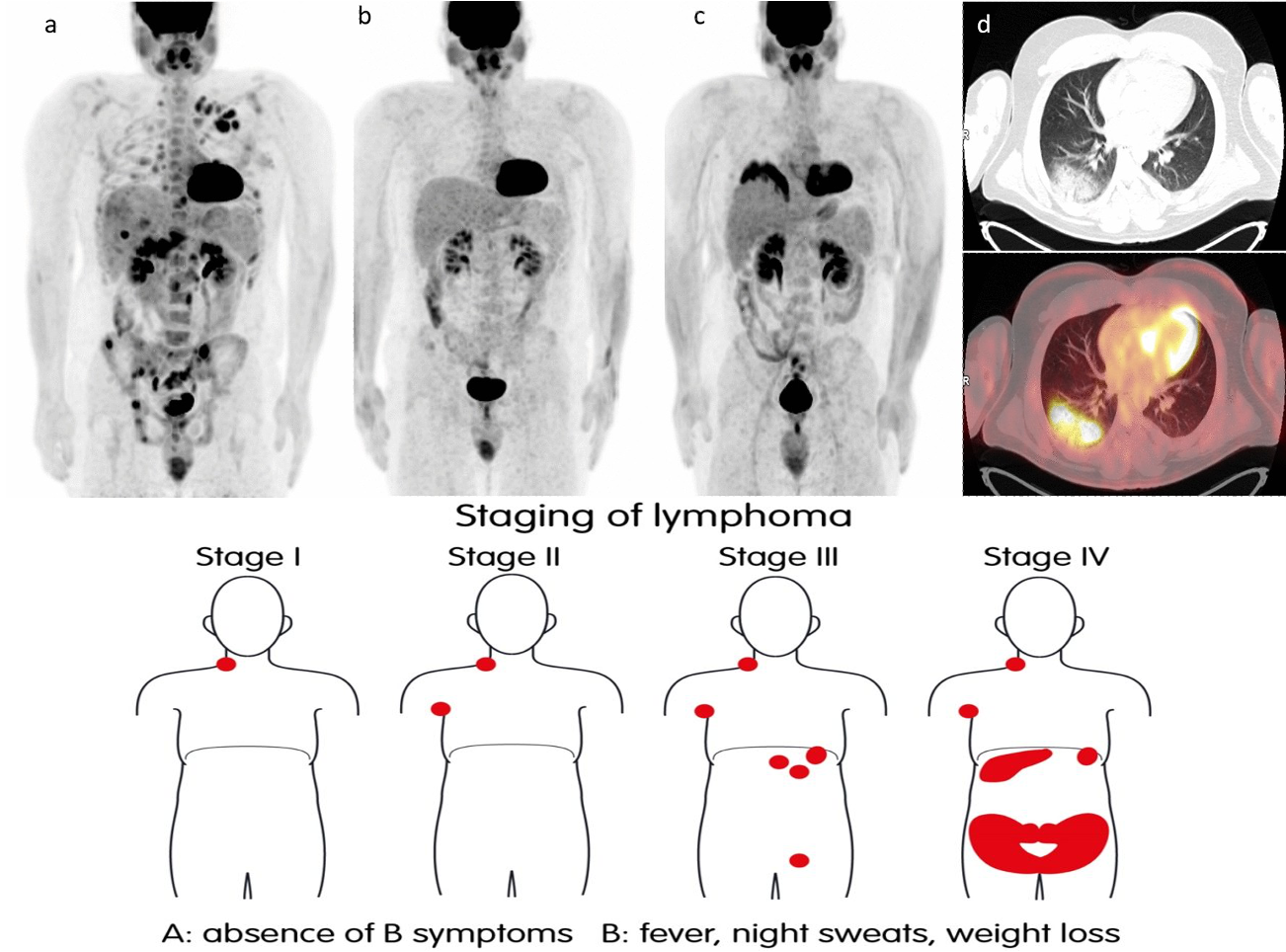
Stages of Hodgkin’s Lymphoma
Based on which lymph node regions are affected:
- Stage 1: Involvement of only one lymph node region
- Stage 2: Involvement of two or more lymph node regions on the same side of the diaphragm.
- Stage 3: Involvement of two or more lymph node regions on both sides of the diaphragm.
- Stage 4: Disseminated disease (involvement of other organs like the liver).
A/B Designation:
-
A: No systemic symptoms (B symptoms)
-
B: Presence of systemic symptoms (B symptoms)
-
Stage 1 A, or 1 B
-
Stage 2 A, or 2 B
-
Stage 3 A, or 3 B
-
Stage 4 A or 4 B
Differential Diagnosis
- Non-Hodgkin’s lymphoma
- Metastases from other cancers
- Infection in the nodes (lymphadenitis); painful
Treatment
-
Radiotherapy: Used alone or with chemotherapy.
- Mantle field (neck, chest, and axilla)
- Inverted Y field (abdomen, spleen, and pelvis)
-
Chemotherapy:
- ABVD (Adriamycin, Bleomycin, Vinblastine, Dacarbazine): Standard initial treatment in the U.S.
- Other regimens: MOPP, Stanford V(5), BEACOPP
- MOPP:
- Mustargen, Oncovin, Prednisone, Procarbazine
- Was used in the past. Rarely used now( only in relapse)
- ABVD:
- Adriamycin, Bleomycin, Vinblastine, Dacarbazine
- Standard initial treatment in the U.S.
-
Stanford V: Contains multiple drugs Used in some countries
-
BEACOPP Contains multiple drugs Used mainly in Europe
Prognosis
Prognosis of HD depends on many factors but overall, it’s a curable cancer in many patients
- Overall 5-year survival rate is 85-90%.
- Poor Prognostic Factors:
- Old age
- Advanced disease (Stage 4)
- Presence of B symptoms
- Large intrathoracic tumor mass